Medical Affairs Catches Fabricated Citations for a Living. Now It's Buying AI That Invents Them.
27% of MSLs now use AI to prep for KOL meetings and only 33% of their companies have a policy. The function built to catch fabricated citations is adopting AI that writes them.
Medical Affairs Catches Fabricated Citations for a Living. Now It's Buying AI That Invents Them.
27% of MSLs now use AI to prep for KOL meetings and only 33% of their companies have a policy. The function built to catch fabricated citations is adopting AI that writes them.

Hospitals Buy Clinical AI Like Software. It Decays Like a Drug.
The Joint Commission started certifying hospitals for responsible AI in June 2026. The standard most will fail is the one that treats a clinical model as a perishable asset, not a one-time install.
Ambient AI Saves One Minute Per Note. Most Health Systems Bought a Different Story.
The largest objective study of ambient AI scribes clocked the gain at one minute per note. Systems that bought it as a productivity play will fail the CFO's test.

AI Can Verify a Prescription. It Still Can't Be the Pharmacist of Record.
Central fill runs error rates below one in a million, yet telepharmacy can't scale past one pharmacist's verify click. The bottleneck is the law, not the tech.

Health Systems Tripled Their AI Spending. Only 4% Have Anything to Show for It.
Hospital CIOs committed $1.4B to AI last year. Only 4% achieved scaled implementation. The problem isn't ambition: it's that 74% are still waiting for Epic to build their AI strategy.

Your Administrative AI Is Working. That's the Problem.
PHTI's April 2026 report found that administrative AI reduces individual transaction costs while inflating system-level spending. The bot wars are live, the upcoding arms race is documented, and most health system ROI dashboards are measuring the wrong variable.

Your AI Rollout Is Deskilling Your Clinicians, and Nobody Is Governing It
Expert endoscopists lost 6 points of cancer detection after months with AI. Deskilling is now measured, and only 22% of health systems govern it.

The DEA Extension Bought Telepharmacy Another Year. Most Programs Are Wasting It.
The DEA's 4th telemedicine extension gives telepharmacy programs a build window through Dec 31, 2026. Most are treating it as a reprieve. Here's the AI workflow strategy that changes the capacity math.

Telepharmacy Moved the Pharmacist Workforce Crisis. AI-Augmented Workflow Redesign Can Fix It.
78.2% of community pharmacists report emotional exhaustion, the highest burnout rate in healthcare. Most telepharmacy deployments moved the crisis, not solved it. Here's the workflow redesign framework that actually changes the outcome.

The Wrong Scorecard: Why Pharmacy AI Keeps Failing the CFO's Test
85% of healthcare AI projects fail before proving value. For pharmacy AI, the problem is a measurement mismatch. Health systems apply ambient-documentation ROI frameworks to cost-avoidance tools, making functioning pharmacy AI invisible at budget time.

OIG Just Flagged AI Coding Prompts as Fraud. Every Health System Using an Ambient Scribe Should Read This.
OIG named AI coding prompts a Medicare Advantage fraud vector. Kaiser paid $556M for the same practice. Here's what ambient AI users must do now.

Ambient AI Skipped the Pharmacist. Here's What That Costs You.
A 2026 npj Digital Medicine study found audio-only ambient AI scribes capture medication strength and form 28% of the time. Most health systems are deploying audio-only platforms anyway.

Utah Overrode Its Medical Board to Keep America's First AI Prescription Program Running. Pharmacies Didn't Get a Vote Either.
On April 28, 2026, Utah dismissed its own Medical Licensing Board's demand to halt the Doctronic AI prescription renewal program. Here's what telepharmacy operators and pharmacy directors need to do now.

The AI Governance Liability Bomb: 75% of Health Systems Are Already Exposed
Three in four health systems have deployed AI. Only 18% have a formal governance policy. This isn't a technology gap. It's an active compliance liability that will be triggered by your next payer audit, regulatory inspection, or patient safety event.
CMS's April 2026 Drug ePA Rule Creates Two-Track Standards, and Most Pharmacy Systems Are Only Built for One
CMS's April 10, 2026 proposed rule separates drug prior authorization into FHIR and NCPDP tracks, with an October 2027 compliance deadline most pharmacy teams aren't planning for.
The FDA Just Made AI Overreliance a Regulatory Violation
The first FDA cGMP warning letter to cite AI misuse as a standalone deficiency landed April 2, 2026. For pharmacy directors running AI in regulated workflows, this is the line of demarcation.

Autonomous AI Prescribing Has Arrived. The FDA Still Hasn't Defined Its Authority.
Utah's Doctronic pilot exposes a jurisdiction gap that no health system is prepared for, and pharmacy is squarely in the middle. Here's what that means for your operations right now.

CMS Just Flipped the Prior Authorization Equation for Drugs
A four-day-old proposed rule forces AI accountability into pharmacy, and the comment window closes June 15, 2026. Here's what every pharmacy director needs to do before then.

The AI Billing Gap: What the 2026 CPT Codes Don't Tell You
CPT 2026 gave healthcare AI its first billing vocabulary. CMS declined to fund most of it. Here is the financial and compliance trap healthcare leaders are walking into.
The Pilot Trap: Why 76% of Healthcare AI Programs Can't Scale, and What to Do About It
Health systems aren't failing at AI because the technology is broken. They're failing because the adoption model they inherited from traditional software procurement doesn't apply to clinical AI.

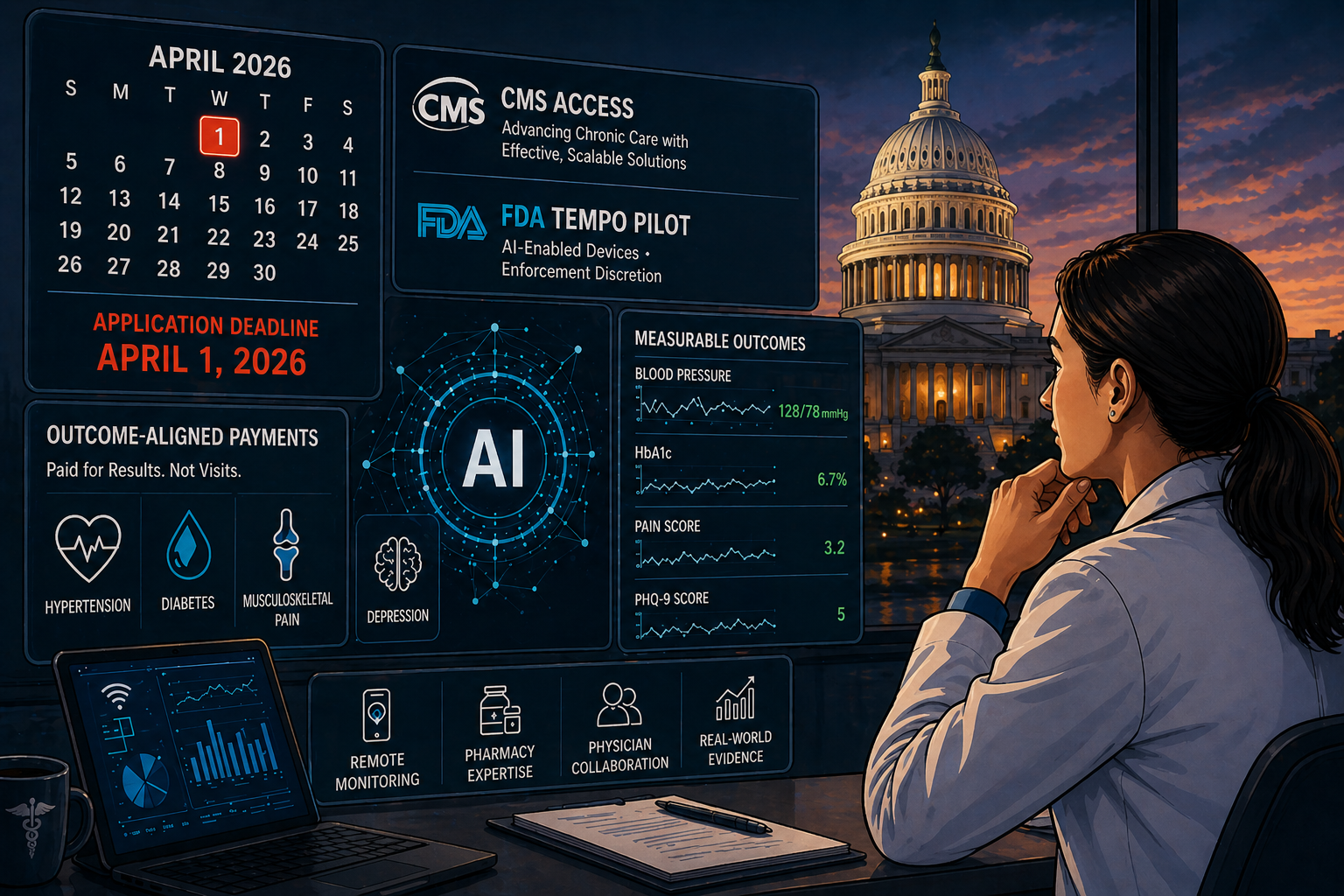
The April 1 Deadline Your Health System Probably Missed
CMS and FDA opened the first outcome-aligned payment pathway for AI-enabled chronic care. Applications close April 1, 2026. Most clinical leaders haven't filed, and most don't know why that matters yet.

Agentic AI Is Reshaping Telepharmacy, and Most Health Systems Are Missing the Play
Walgreens fills 60% of prescriptions with robotics. CVS deploys AI across 9,000 locations. Yet 81% of hospital pharmacy operations haven't adopted AI at any level. The gap isn't a technology problem. It's a strategic framing problem.

FDA's 2026 CDS Guidance Makes Transparency Non-Negotiable: What Telepharmacy Operators Must Do Now
The FDA's January 2026 Clinical Decision Support guidance dismantles the black-box era in clinical AI. For telepharmacy operators, the compliance window is already open.
Why Most EHR-Integrated AI Tools Fail at the Point of Care, and What Actually Works
Clinicians in AI-enabled health systems are receiving up to 200 alerts per day. They override 96% of them. The problem isn't the AI. It's the integration strategy.